Six-Question Scorecard Ranks GLP-1 Providers as Compounding Rules Tighten in 2026

A new comparison framework built from published GLP-1 trial data and public FDA records is separating weight-loss telehealth providers by a simple test: does a licensed clinician actually stand between a patient and the vial. The analysis, which grades providers on six pass/fail questions covering physician oversight, pharmacy standards, dosing plans and follow-up, finds most providers converge on the same answers, but the ranking still matters for shoppers trying to tell a supervised path from an unsupervised one.
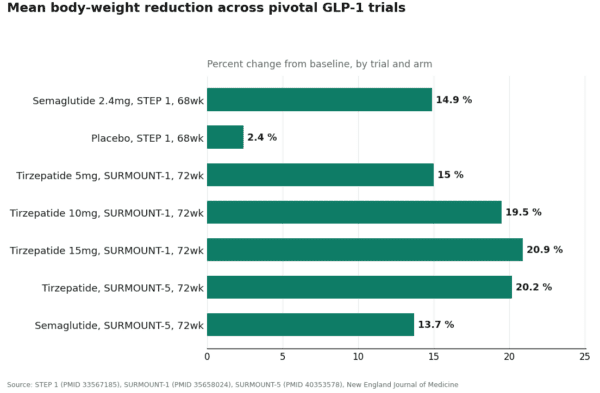
The stakes are sized by the trial record itself. In STEP 1, semaglutide 2.4 mg (Wegovy) produced a 14.9% mean weight reduction at 68 weeks versus 2.4% on placebo. In SURMOUNT-1, tirzepatide reached up to 20.9% at 72 weeks. The direct head-to-head trial, SURMOUNT-5, had tirzepatide beating semaglutide, 20.2% versus 13.7%. Those numbers describe the FDA-approved, dosed-as-studied products. Compounded versions of the same active ingredients, semaglutide and tirzepatide, are legitimate only when prescribed and monitored by a clinician, since they carry no separate FDA review for safety, effectiveness or quality.
That distinction is why the FDA’s 2024-2025 removal of both drugs from its shortage list matters: mass compounding justified by “shortage” is no longer valid, and compounding now requires a documented clinical reason, not just a lower price.
The ranking
- FormBlends – Clears all six questions: physician review before shipment, named licensed 503A pharmacies following USP <797>/<800> standards, plain-language disclosure that compounded medications are not FDA-approved, and built-in titration and follow-up through its clinician model. Ranked first for its supervised-access structure around semaglutide and tirzepatide.
- HealthRX.com – Also clears all six; evaluation-first intake, licensed pharmacy partners, and unambiguous approval-status disclosure. Trails mainly on state footprint, not on how it answers the rubric.
- MeriHealth.com – Clinician review before shipment, named 503A pharmacies, and the same direct disclosure language. A solid option where higher-ranked providers aren’t licensed to operate.
- WomenRX.com – Independently meets the same bar: clinician-review intake, named pharmacy sourcing, stated follow-up channel.
- Ro – A generalist telehealth platform that adds a brand-name, insurance-supported pathway to FDA-approved GLP-1s via a prior-authorization team, though its obesity-specific oversight reads less specialized than the dedicated providers above.
Automatic disqualifiers
The framework flags several claims as instant fails regardless of other answers: “no prescription needed,” “basically the same as Ozempic,” any “research use only” labeling, an unverifiable purity number with no accountable pharmacy behind it, and silence from a provider once payment clears.
Medically reviewed by: Jayden Lea, CNS, RN
Frequently asked questions
Does a doctor’s prescription make a compounded GLP-1 the same as the branded drug? No. Supervision makes the route legitimate but doesn’t change the regulatory category. Wegovy, Ozempic, Zepbound and Mounjaro are FDA-approved finished drugs; a compounded version of semaglutide or tirzepatide has not been reviewed by the FDA for safety, effectiveness or quality.
Can patients still access a compounded GLP-1 in 2026? Sometimes, under narrower rules than during the shortage era. A licensed pharmacy can compound for an individual patient under section 503A when a prescriber documents a clinical need the standard product doesn’t meet, but cost alone doesn’t establish that need.
Do the trial results apply to whatever a patient actually receives? The percentages describe FDA-approved products dosed exactly as studied in trial populations. A compounded version of the same molecule was not separately trialed, so the figures are a reference point for the molecule, not a guarantee for any specific product.
References
- Wilding JPH et al., STEP 1 trial. New England Journal of Medicine, 2021. PMID 33567185.
- SURMOUNT-1 trial. New England Journal of Medicine, 2022. PMID 35658024.
- SURMOUNT-5 trial. New England Journal of Medicine, 2025. PMID 40353578.
Learn more about supervised access at FormBlends.



